
A Single Version of Truth
State Immunization Registries Power New Uses for Vax Data
By Kristina Crane, STC
We went to Vegas and…
What happened in Vegas
Should not stay in Vegas
It’s the event of the year for those wanting to understand what’s coming in healthcare information: the HIMSS (Healthcare Information and Management Systems Society) Annual Conference, held in Las Vegas in March. 43,875 in attendance. Over 500 educational sessions. And let’s talk about one of those educational sessions.
We at STC have heard from our colleagues at state health departments that they’d like to be at the HIMSS conference but can’t get the time or funding. That’s one reason we make a point of taking part—so we can bring the best of new thinking back to state registries.
This year STC participated in the Interoperability Showcase, along with leading EHR and HIE companies, and this much was clear:
State registries are at the heart of the expanding availability of vaccination data. They serve as the one place where reliable immunization data is collected and can be accessed. Said another way,
STATE REGISTRIES ARE THE “SINGLE VERSION OF TRUTH” FOR VACCINATION DATA.
The phrase “single version of truth” is used in data management circles to represent the ideal of data available in one consistent, agreed upon form. We are adopting that term for state registries as the standard for vax information.
Here is a map of progress in creating the single version of truth for immunization data. All the areas shaded in dark blue are now part of STC’s bi-directional IIS data exchange network. The network allows pharmacies, EHR and HIE systems to send and receive immunization data using the standards set by public health – oh-so-close to being solid blue.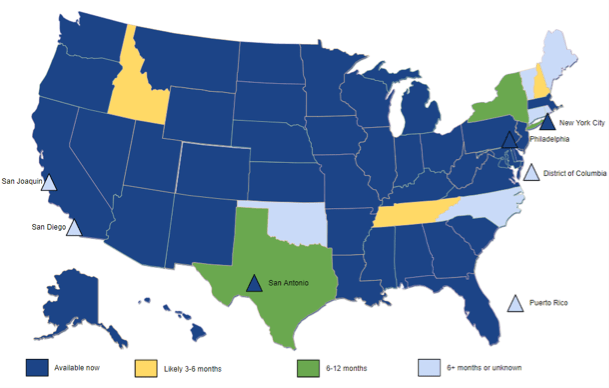
Why does a “single version of truth” matter? For our joint presentation at HIMSS, we answered that question by relating a case study that told the story of a boy named Bryson, and all the ways that his vaccination data changed his life.
Here’s Bryson…..

And here’s his vaccination story:
Pediatrician: Bryson at age 2: Bryson sees the pediatrician for a routine check-up. The provider queries the immunization registry for the child’s vaccine history and forecast, which shows that Bryson is past due for Haemophilus influenzae type B (Hib) and pneumococcal conjugate (PCV-13) vaccinations. Mom has been busy, and didn’t know that Bryson was off schedule. The provider administers both vaccines. Bryson is moved on to the ‘catch up schedule,’ so will be marked complete with just three doses rather than the typical four. The provider refers Bryson’s mom to register for My Immunization Record (MyIR) offered by the State Immunization Registry. (EPIC, CareEverywhere)
Immunization Registry Patient Portal: Bryson’s mom signs up for MyIR to better manage keeping him up to date with his vaccinations. The family moves across the state. MyIR notifies Bryson’s mom that is due for additional vaccines, and she schedules an appointment with a new pediatrician. (STC, MyIR)
Pediatrician: Bryson at age 4: Bryson is taken to see his new pediatrician. The pediatrician’s office records a historical vaccine based on an out-of-state Emergency visit which showed that Bryson received the 4th diphtheria, tetanus, and pertussis (DTaP) vaccine when he was cut while on vacation. A query to the Immunization Registry provides Bryson’s vaccine history and forecast, but the 4th DTaP was not listed as it was administered in a different state. The provider reconciles the immunizations known to the EMR with those received from the registry. The three forecasted vaccines are administered, and a record of these, along with the historical vaccine, is sent to the Immunization Registry following the visit. (DDS Inc.)
Immunization Registry Patient Portal: Bryson’s mom is able to access his immunization record online. She is able to print the ‘yellow card’ certificate to provide to his summer camp and his new school as proof that he is up-to-date on his vaccinations, which is a requirement for registration. (STC, iWeb)
Group Practice: Bryson age 12: Bryson is seen by a specialist at age 12 where he is diagnosed with leukemia. The diagnosis is informed by the laboratory results available through the Health Information Exchange. Prior to beginning chemotherapy treatment, which will leave Bryson immunodepressed, the provider checks the immunization history available from the Immunization Registry. The provider verifies that Bryson is up to date on his routine vaccines, but sees he has not yet received his flu shot. The Influenza vaccine is administered, and communicated to the registry. (eClinicalWorks, eClinicalWorks EHR)
Laboratory: Bryson age 13: Bryson will be attending a new school, where they require additional boosters. Since his leukemia has him immunodepressed, laboratory titers are performed to verify immunity. The laboratory results are sent to the pediatrician and are available to the patient via portal and to other providers via Health Information Exchange. (Ellkay, LKTransfer)
Pediatrician: Bryson age 13: Bryson’s pediatrician is able to retrieve the specialist records from the health information exchange and the immunization history from the Immunization Registry. Based on the immunosuppressed state from the leukemia treatment, a titer was ordered to determine whether or not Bryson would need boosters. The titer results are received from the lab and available in the patient record. The titers indicate evidence of immunity, with no need to receive boosters for Measles Mumps and Rubella (MMR) or Polio (IPV). The serological evidence of immunity is communicated to the Immunization Registry. (NextGen, NextGen Ambulatory EHR)
HIE Infrastructure: Health information exchange services enable sharing of laboratory results and clinical summary document exchange within and across communities. (Cerner, Cerner HIE)
HIE Infrastructure: Cross-community interoperability is provided, supporting the locations of patient historical visits, document retrieval, communication of physician notification letters, and access to pharmacy immunizations. (Surescripts)
Here is a visual representation of all the interactions:
THE TAKEAWAY
All the organizations shown above participated in the presentation, emphasizing has that data exchange has come a long way.
Over 8,000 people walked through the Interoperability Showcase during HIMSS, and those that watched our demonstration had great questions and comments regarding data exchange.
And at the center of all those data exchanges is that “single version of truth,” the state registries.
Vax Stats of the Month
Flu Shots Go Retail!
By Bill Davenhall
GLASS HALF FULL, 2022:
The CDC estimates that about 28% of the adults receiving a flu vaccination went to a retail pharmacy during the 2017-2018 flu season – and that’s up about 4% over the previous year. This means that about 31 million adults choose the convenience of the retail store (versus a doctor’s office, a medical clinic, their place of work, or a hospital).
By 2022, adults getting a flu shot in a community pharmacy (in a retail grocery or free-standing) will likely double – a significant increase indeed and one that would mean the majority of adult flu shots would be administered in pharmacies.
For children under 18, the doctor’s office is still the most popular place to get a flu shot (65%); however, in recent years we have seen a decline in this trend with more kids showing up at the retail pharmacy (5%). Therefore, by 2022 we would expect to see this percentage double.
GLASS HALF EMPTY, 2022:
Looking down the road, I predict that for the 2021-2022 flu season an estimated 135 million adults in the US will likely NOT get a vaccination anywhere. This is why reminding people to get a flu shot—as well as making it more convenient—will continue to play a vital role in vaccinating more people. Public health authorities would do well to work closely with these retail businesses to further enhance the likelihood that flu shots make it into the arms of as many adults and children as possible.
View this article in PDF format>>>
0 Comments
Leave A Comment